The most important reason for performing joint fluid analysis is to rule out septic arthritis. Synovial fluid analysis can demonstrate local inflammatory response, infection and the presence of crystals. Synovial fluid effusions are classified into five general etiologic categories: noninflammatory responses, inflammation, sepsis, crystal induced and hemorrhage. The most common diseases associated with each category are summarized in the following table.
The following tests can be performed on synovial fluid.
Synovial fluid protein concentration is usually 25% of serum (1-3 g/dL). Synovial fluid glucose is normally within 10 mg/dL of plasma glucose. Neither synovial fluid glucose nor protein provides much useful diagnostic information. White cell counts (WBC) are normally less than 200/uL with fewer than 25% neutrophils. A WBC count of 2,000/uL and a neutrophil count of 75% serve as useful cutoff points to distinguish inflammatory from noninflammatory disease. However, there is much overlap in synovial fluid WBCs between the inflammatory, crystal-induced, and sepsis categories. WBC is greater than 50,000/uL in 70% of patients with septic arthritis, 15% with gout, 10% with pseudogout, and 4% with rheumatoid arthritis. Acute septic arthritis is usually caused by bacterial infection of the joint. Tuberculosis and fungi are less commonly involved. Infection can occur by hematogenous spread, direct innoculation during surgery or trauma or from osteomyelitis. Septic arthritis is usually characterized by an acute onset of monoarticular joint pain. Staph aureus is responsible for the majority of cases of bacterial infection. Neisseria gonorrhea is common in adolescents and young adults. E. coli is most commonly seen in neonates. Other gram positive rods are associated with immunocompromised patients. Specimen requirement for cell count and differential is 1 mL of synovial fluid transferred to a lavender top (EDTA) tube. Bacterial cultures require 2-3 mL of fluid in a yellow top tube. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Sunday, July 20, 2008
Synovial Fluid Analysis
mrcp,rheumatology
30 years old male got acute left knee arthritis with swelling.it gradually resolving for 2 months and now he got acute swelling and tenderness in right knee.no history of eye redness or dysuria.no history of gonococcal urethritis.no back pain.
mrcp,rheumatology
A 30 year-old man is admitted to casualty with a 24 hour history of a painful and swollen right knee. He denies any previous history of joint problems. Over the last two days, he has also noticed redness and soreness in both eyes. He has returned from a business trip to Kuala Lumpur a fortnight ago.
On examination, his temperature is 38.5°C. His eyes are red. His right knee is hot, swollen and tender to palpate. No other joint appears to be affected.
Investigations:
Hb 12.9 g/dl
WBC 14.0 x 109/l
Platelets 200 x 109/l
ESR 75 mm/h
Blood cultures
No growth after 48 hours
Urinalysis
No blood, glucose or protein detected
Knee x-ray
Soft tissue swelling around left knee
What is the most likely diagnosis?
1 )Gout
2 )Gonococcal arthritis
3 )Reiter's syndrome
4 )Rheumatoid arthritis
5 )Viral arthritis
On examination, his temperature is 38.5°C. His eyes are red. His right knee is hot, swollen and tender to palpate. No other joint appears to be affected.
Investigations:
Hb 12.9 g/dl
WBC 14.0 x 109/l
Platelets 200 x 109/l
ESR 75 mm/h
Blood cultures
No growth after 48 hours
Urinalysis
No blood, glucose or protein detected
Knee x-ray
Soft tissue swelling around left knee
What is the most likely diagnosis?
1 )Gout
2 )Gonococcal arthritis
3 )Reiter's syndrome
4 )Rheumatoid arthritis
5 )Viral arthritis
erythema nodosum,mrcp


Very frequent MRCP exam question, especially Part 1 & 2a, don't be surprised if it comes out in Station 5 PACES.
The picture shows erythematous nodules over the legs involving the shin. They are tender and elevated.
My diagnosis is that this patient has erythema nodosum.
You need to know the causes !
May even appear in history taking if you read Mir &Ryder PACES
Idiopathic/ unknown
Sarcoidosis
Streptococcal infection
Tuberculosis
Infections other than TB or strep - HIV...
Pregnancy or oral contraceptives
Drugs other than OCAs
Inflammatory bowel disease
Behcet's disease
Other
massive splenomegaly.+mrcp
Box 1 Diseases that cause massive splenomegaly.
- Chronic myeloid leukemia
- Extrahepatic portal vein obstruction
- Gaucher's disease
- Hairy-cell leukemia
- Idiopathic portal hypertension
- Malaria
- Malignant lymphoma
- Myelofibrosis
- Thalassemia major
- Visceral leishmaniasis (i.e. kala azar)
sarcoidosis in mrcp
They would usually show show you a CXR in MRCP
Remember that 90% of CXRs have bilateral hilar LN enlargement. More advanced case may have diffuse fibrosis!
Tips for MRCP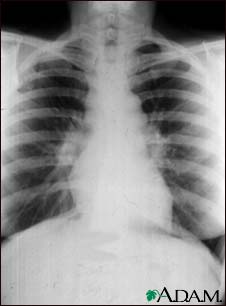
Remember that 90% of CXRs have bilateral hilar LN enlargement. More advanced case may have diffuse fibrosis!
Tips for MRCP
1) If you are asked about a patient with painful skin lesions over shin area with dry cough, always think of sarcoidosis.
2) A patient with high calcium level and dry cough , think of sarcoidosis although there is possibility of lung cancer with bone metastasis!
- Stage 0 is a normal chest x-ray.
- Stage 1 is a chest x-ray with enlarged lymph nodes but otherwise clear lungs.
- Stage 2 is a chest x-ray with enlarged lymph nodes plus
infiltrates (shadows) in the lungs. - Stage 3 is a chest x-ray that shows the infiltrates (shadows) are present but the lymph nodes are no longer seen.
- Stage 4 shows scar tissue in the lung tissue.
Subscribe to:
Comments (Atom)


